The NYIHR Position on Stem Cell Therapy

What Is So Special About Stem Cell Research?
Stem cell research goes back to the 1950s when German biologist, Ernst Haeckel coined the term. In the United States, while working with adult mice, in cancer research in Bar Harbor, Maine, researcher Leroy C Stevens discovered these cells could change into any cell (pluripotency).
By 1998, after 50 years of study and research, scientists learned how to take stem cells from a human embryo and grow them in a laboratory. That became an ethical football. Religious leaders and ethics philosophers rallied the support of politicians to prevent research. They expressed deep concern scientists would encourage the harvesting of the newly-born and unborn to solve adult health problems.
Researchers turned their focus to adult stem cells. While adult cells are not as powerful as embryonic cells, they can be taken from one part of one’s body and used to heal another part in sufficient numbers. Stem cell research continued with a new challenge – overcoming the decreased ability to change into as many other types of cells during development. Hence, the preference for younger stem cells.
Stem cells are attractive to medical professionals because they can heal many diseases caused by the loss or malfunction of cells in our bodies. Since stem cells can match and multiply into other types of cells, we have hope we can reverse diseases we cannot currently cure. Studies are underway in areas of cancer, type-1 diabetes, and chronic lymphocytic leukemia. A more common and successful approach is in healing soft tissue with adult stem cells. Knees, shoulders, wrists, and hands are typical candidates for stem cells in the emerging field of regenerative medicine.
How Does It Work?
The following example relates to typical candidates. In this process, the stem cell treatment endorsed by our institute applies stem cells to a three-dimensional network of extracellular macromolecules (ECM Matrix). We use hyaluronic acid (HA) to reproduce the tissue microenvironment. Using HA in a 3D system allows a more dense and compact cellular environment.
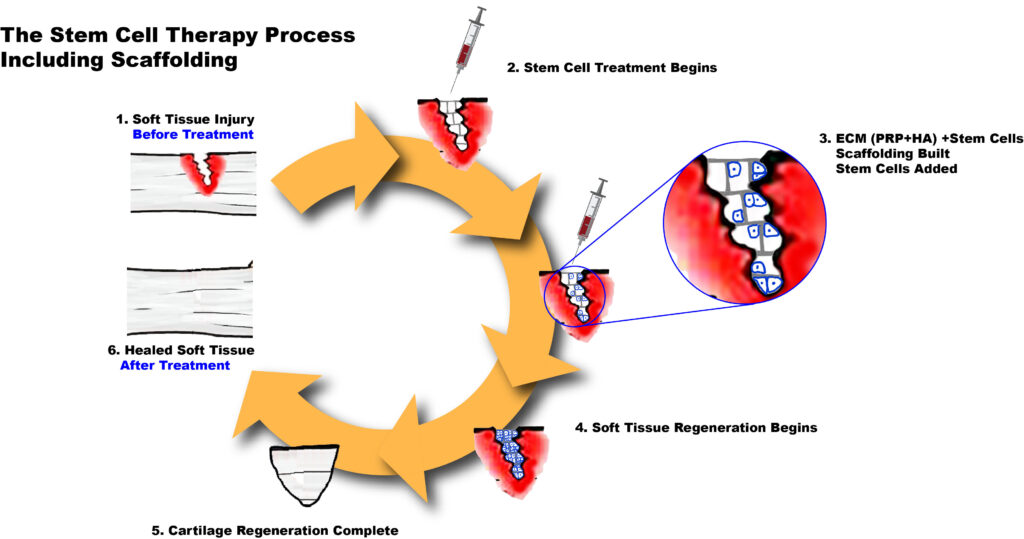
The diagram above has six key events.
1. Soft Tissue Injury
After we determine that the cartilage (tendon, ligament or meniscus) has a “partial” tear we begin the treatment plan to regenerate the tissue. This diagnostic step is critical because it helps us make the decision whether we need to recommend surgery (for “complete” tears) as opposed to a more conservative approach using regenerative medicine like stem cell therapy.
2. Stem Cell Treatment Begins
Once the patient is accepted as a candidate for stem cell therapy, we begin by injecting a combination of Extracellular Matrix (ECM), Hyaluronic Acid (HA), Platelet-Rich Plasma (PRP) along with stem cells into the injured joint. This procedure is always done under ultrasound guidance.
3. ECM (PRP+HA) + Stem Cells Scaffolding Built
The combination of Extracellular Matrix (ECM) and Hyaluronic Acid (HA) may work as a scaffold where stem cells can attach and begin to divide and grow.
The Platelet-Rich Plasma (PRP) contains important Growth Factors (GF’s) necessary for the survival, division and growth of the stem cells.
4. Soft Tissue Regeneration Begins
The stem cells begin to actively divide, grow and differentiate along the scaffold into new soft tissue known as cartilage (tendon, ligament or meniscus).
5. Regeneration Complete
The stem cells undergo complete differentiation to become newly regenerated cartilage.
6. Fully Healed Soft Tissue
The previously injured cartilage is now fully healed.